In new research published in Neuron this week researchers from Brown University in Providence, RI suggests that disruption of the circadian rhythm protein CLOCK alters cortical circuits and may lead to generation of focal epilepsy.
Dr. Liu and her colleagues used resected brain tissue from epilepsy surgery for focal cortical dyplasias and analysed the tissue's transcriptome, or a survey of the messenger RNA (mRNA) in any given population of cells. They used adjacent healthy tissue as controls.The researchers were looking at differences between healthy and epileptogenic tissue and to their surprise found that there was a decrease in the expression of mRNA coding for a protein called circadian locomotor output cycles kaput (CLOCK) in the epileptogenic tissue.
CLOCK is a key player in the regulation of our circadian rhythms. Mice with mutated versions of the gene are unable to maintain normal daily rhythms of sleep and wakefulness. In the unhealthy brain tissue from participants with epilepsy, CLOCK was reduced in both excitatory and inhibitory neuron. CLOCK is important for regulating a range of genes and other CLOCK-associated proteins were also absent or reduced in the brain tissue.
To investigate this further the researchers generated and tested separate knock out mouse models with targeted deletions of the CLOCK gene in excitatory and inhibitory neurons. They found that the mice without CLOCK in their excitatory neurons showed symptoms of epilepsy similar to those in the human patients, including an increased susceptibility to seizures - especially when waking up.
They also found that excitatory neurons that lacked CLOCK received less inhibitory inputs from surrounding cells, in effect unleashing them and potentially giving them a lower threshold for the onset of seizures. The findings will certainly put more focus on the role of CLOCK in the molecular mechanisms behind epilepsy.
Citation: Li P, Fu X, Smith NA, Ziobro J, Curiel J, Tenga MJ et al. (2017) Loss of CLOCK Results in Dysfunction of Brain Circuits Underlying Focal Epilepsy.Neuron 96 (2):387-401.e6. DOI: 10.1016/j.neuron.2017.09.044 PMID: 29024662.
Read More
- Details
- ICNA
- News
- Hits: 1394
In a paper just published online in the journal The Lancet, Craig McDonald and colleagues at 53 study sites in 18 countries describe the clinical benefit of using the drug ataluren for a certain group of patients carrying a specific "nonsense mutation" for Duchenne muscular dystrophy.
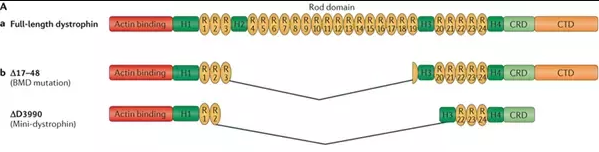
Duchenne muscular dystrophy (DMD) is a progressive and life-limiting X-linked recessive disorder caused by mutations in the DMD gene that result in reduced or absent dystrophin production. Dystrophin is part of the dystrophin–glycoprotein complex, which acts as a scaffold between the actin cytoskeleton and the extracellular matrix and, as such, maintains muscle fibre integrity.
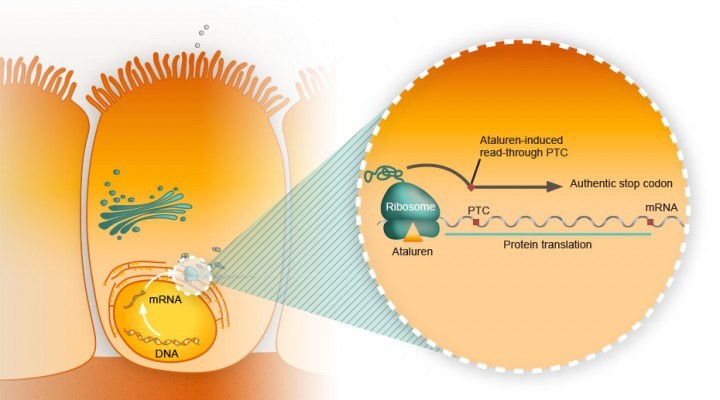
A single nucleotide change in the DNA sequence that introduces a premature stop codon is known as a nonsense mutation, a subset of a major class of premature termination codon (PTC) mutations. Nonsense mutations cause premature termination of translation resulting in the production of truncated polypeptides, which in turn halts the ribosomal translation process at an earlier site than normal, producing a truncated, non-functional protein. Ataluren makes ribosomes less sensitive to premature stop codons (referred to as "read-through"). Ataluren allows for those premature stop codons to be read through and complete the protein:

Ataluren has been marketed under the trade name Translarna by PTC Therapeutics (South Plainfield, NJ, USA). The drug allows ribosomal readthrough of premature stop codons, thus enabling production of functional dystrophin that might ameliorate disease progression.
The study, a phase 3, multicentre, randomised, double-blind, placebo-controlled trial (ACT DMD) was sponsored by the New Jersey-based company that developed ataluren, PTC Therapeutics. It included 230 patients, half of whom received the drug therapy over a course of 48 weeks, and the other half who received a placebo.
It assessed the ability of ataluren to stabilise ambulation, with a focus on a prespecified subgroup of patients with ambulatory decline. The primary endpoint of change in 6-min walk distance (6MWD) from baseline to week 48, with a hypothesis of a difference of at least 30 m between ataluren-treated and placebo-treated patients, did not differ significantly between groups in the intention-to-treat population.
Duchenne study participants with the nonsense mutation who had a baseline six-minute walk of between 300 meters and under 400 meters were the subgroup of patients who were the most likely to see the clinical benefits of ataluren.
ACT DMD and the use of ataluren provide a glimmer of hope for the approximately 10–15% of patients with DMD have an underlying nonsense mutation in the DMD gene 2 where the drug seems to prompt a slowing or stabilizing of the disease progression and motor function.
In 2016, the European Medicines Agency gave conditional approval for the drug to be used and, once data demonstrating its ability to stabilise ambulation were obtained, the National Institute for Health and Care Excellence (NICE) agreed reimbursement within a managed access agreement for the treatment of ambulant patients with DMD aged 5 years or older.
Other therapeutic approaches are currently being trialled in patients with DMD, several of which are mutation specific. These approaches include the use of compounds facilitating the upregulation of dystrophin analogues (NCT02858362); exon-skipping techniques with antisense oligonucleotides to convert an out-of-frame mutation into an in-frame mutation, thus allowing partial dystrophin expression; and the use of selective steroid receptor modulators (NCT02760264).
Ataluren in patients with nonsense mutation Duchenne muscular dystrophy (ACT DMD): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial, Craig M McDonald et al., The Lancet, doi: 10.1016/S0140-6736(17)31611-2, published 17 July 2017.
Wood CL, Cheetham T (2017) Treatment of Duchenne muscular dystrophy: first small steps.Lancet():. DOI: 10.1016/S0140-6736(17)31669-0 PMID: 28728957.
Read More
- Details
- ICNA
- News
- Hits: 1752

At the Amsterdam ICNC in May 2016 interested members of the ICNA met to discuss a way forward to provide support for trainees and newly qualified child neurologists (within 5 years)
Direction of how to learn and what to learn for trainees
Educational meetings – especially focused on-site educational meetings
How to put a grant together (Plan a symposium at the next ICNC2018 on this)
Support from the EB with guidance on projects – developing viable protocols
Big support for need for fellowships to support skills development in RPS
On-line training resources – identify and support ICNApedia as a resource and portal
Promotion of telemedicine to discuss complex cases
Guidance from established ICNA members on career development to trainees before taking up permanent posts and losing the capacity to adjust career path. Distance mentorship would avoid a conflict of interest but may need to include individuals from same country who know the local system best.
Learn how to advocate for patients and for what is needed for the profession (Plan a session at ICNC2018)
A working group need to be elected. This group would predominantly hold "virtual meetings", communicating via e-mail and skype and coming together at opportunistic meetings which they would be attending routinely e.g. ICNCs. The lead for this working group will be funded to attend the ICNA EB meetings (once a year) to feedback progress and developments in the program.
We call for nominations for members who would like to be part of this committee. There will be regional representation and the committee will rotate every 4 years. Two doctors from each of the ICNA regions (Africa,
Eastern Asia-Oceania, Europe, North America, South America, West Asia) will be elected to the committee. The person with the greatest number of votes will be the leader.
Please complete the online form if you would like to submit your nomination.
Read More
- Details
- ICNA
- News
- Hits: 1285
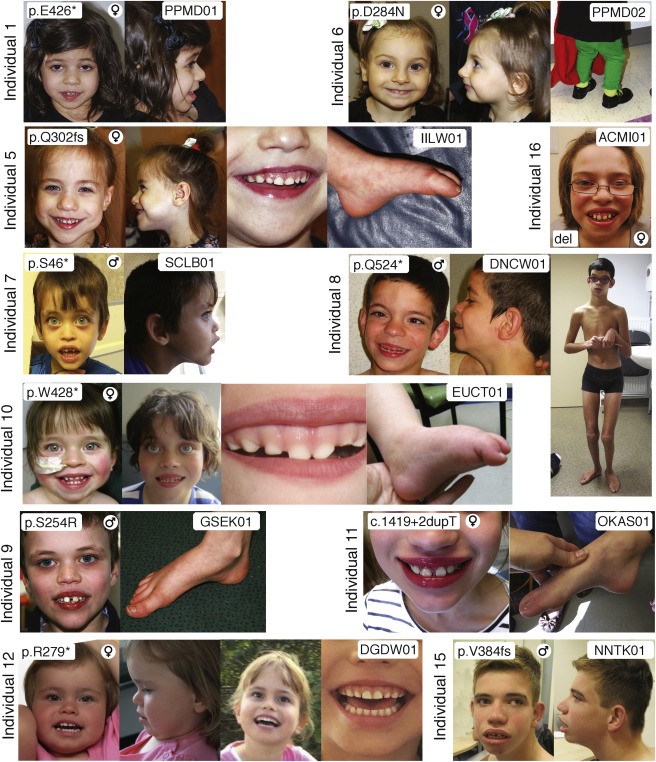
Researchers at Children's Hospital of Philadelphia (CHOP) have pinpointed variants in the WDR26 gene to a rare syndrome characterized by intellectual disability, seizures, an abnormal gait and distinctive facial features. In a study published in the American Journal of Human Genetics Deardorff, first author Cara M. Skraban, MD, also of CHOP, and co-authors from medical centers in six countries reported on 15 individuals now known to have this recognizable syndrome. Prior to this it was not even listed in some of the most commonly used databases.
The affected individuals ranged from two years old to 34 years old. All the patients had developmental delays (ranging from mild to severe), seizures, and similar facial features (such as wide mouths, prominent upper lip and gums, full cheeks and a broad nasal tip). Many had subtle abnormalities in their gait. All 15 had de novo (new) mutations - those arising in a single egg or sperm that developed into the affected patient, but did not occur in the patient's parents.
CHOP has started a patient registry to compile clinical data on this rare condition (see This email address is being protected from spambots. You need JavaScript enabled to view it.). The data collection may offer a resource for families interested in contacting each other to share information and support.
Source: WDR26 Haploinsufficiency Causes a Recognizable Syndrome of Intellectual Disability, Seizures, Abnormal Gait, and Distinctive Facial Features, Cara M. Skraban et al., American Journal of Human Genetics, doi: 10.1016/j.ajhg.2017.06.002, published 6 July 6 2017.
Read More
- Details
- ICNA
- News
- Hits: 1378

The International Child Neurology Association (ICNA) is deeply saddened to hear the passing of Isabelle Rapin, MD. Dr Rapin, a true giant in the field of child neurology has helped found the International Child Neurology Association and has been a staunch supporter of its activities and ICNApedia all her life.
Dr Rapin was a member of the first executive board of the ICNA (1973–1975) and Chairman of the Program Committee for the first ICNA Congress October 6–10, 1975 held in Toronto.She was also the recipient of the ICNA Frank R. Ford Award in 1990 and delivered her Lecture on "Autism as a neurological disorder" at the Toronto congress in 1990. She had previously received the Hower award from the Child Neurology Society, USA in 1987. Dr Rapin's other awards and recognitions include the President's Award from the American Academy of Neurology, Honorary Alumna status from the Albert Einstein College of Medicine, Award for Excellence in Autism Research from the Autism Society of America and the Shriver Center Award.
According to Dr Kenneth J. Mack, current President of the Child Neurology Society (CNS) and Executive Board Member of the ICNA the breadth and depth of Dr Rapin's knowledge was exceeded only by her collaborative spirit and her unfailing willingness to engage younger colleagues in conversation who sought her wise counsel at Einstein Medical Center or at any number of national and international meetings.
The New York Times said: "Considered by many the doyenne of autism, Dr. Rapin has spent decades studying the disability." while the Boston Globe described her as a
"leading authority on autism". She was a fellow of the American Academy of Neurology (FAAN).
She was a professor emerita in both the Saul R. Korey Department of Neurology and the Department of Pediatrics at the Albert Einstein College of Medicine in New York City from where she retired in 2012, at the age of 84.
 Dr. Rapin receiving her Honorary Alumna award at commencement, in 2000, from Dr. Dominick P. PurpuraIn an autobiography published in the Journal of Child Neurology in 2001, She said:
Dr. Rapin receiving her Honorary Alumna award at commencement, in 2000, from Dr. Dominick P. PurpuraIn an autobiography published in the Journal of Child Neurology in 2001, She said:
"The message I would give a young colleague is that child neurology is a wonderfully rewarding field, intellectually and personally, because of the families you will meet. In order to have it all, that is, be married, have children, restore and furnish an antique house, work in the garden, enjoy a lot of what life offers, and have a great job, you need a supportive and generous mate, adequate baby sitting and house help, flexibility, good humor, and a nose for the unusual. Consider every patient a potential source of new knowledge, describe what you see, pursue your interests vigorously, and learn to cut corners and prioritize. Find a good mentor, enjoy what you do, and be lucky."
Dr Rapin along with Dr Roberto Tuchman edited the ICNA IRCN series title "Autism: A Neurological Disorder of Early Brain Development" in 2006. Some of her other works include
- Riva D, Rapin I, Zardini G (2006). Language: Normal and Pathological Development. John Libbey Eurotext Ltd. ISBN 978-2472006384.
- Rapin I (1996). Preschool Children with Inadequate Communication. MacKeith Press. ISBN 978-1898683070.
- Rapin I (1994). Handbook of Neuropsychology. 6. Elsevier Science Ltd. ISBN 978-0444820600.
- Rapin I (1982). Children with Brain Dysfunction: Neurology, Cognition, Language, and Behavior. Raven Press. ISBN 978-0890048443.
- Haas RH, Rapin I, Moser HW (1988). Rett Syndrome and Autism. Year Book Medical Pub. ISBN 978-9990808179.
In addition she has authored more than 135 papers and 75 book chapters. One of her latest contributions to ICNApedia was an article she wrote following the news of the demise of Dr Masaya Segawa titled "2014: Passing of the Guard in International Child Neurology".
With her passing, the International Child Neurology Community has lost yet another true great, but her legacy and teachings will live for ever through the work of the associations she helped build and the countless students and colleagues she had mentored.
See also:
- Dr. Isabelle Rapin: A Living Legend
- Rapin I (1999) The International Child Neurology Association: the first 25 years.Brain Dev 21 (1):3-15. PMID: 10082246.
- 2014: Passing of the Guard in International Child Neurology
- Reminiscences of a 52-year member of the Saul R. Korey Department of Neurology at Einstein
- Details
- ICNA
- News
- Hits: 3318