Fever induced refractory epileptic encephalopathy in school age children (FIRES) is a devastating condition which follows a prolonged refractory status epilepticus (SE) triggered by fever of unknown cause. The intractable perisylvian status epilepticus might persist for more than a month and results in severe cognitive impairment.
History
Several authors[1][2][3][4][5] have reported a presumed post encephalitic catastrophic epileptic encephalopathy resulting in refractory repetitive seizures associated with severe cognitive impairment.
Mikaeloff et al[3] in 2006 described this condition in a retrospective study of normally developing 14 children (mean age 7.5yrs) admitted with prolonged status epilepticus following a nonspecific febrile illness and called it Devastating Epileptic encephalopathy in School-age Children (DESC).
The current term febrile infection-related epilepsy syndrome (FIRES) was proposed by Van Baalen et al[6] in 2010 who published a retrospective multicenter case series of 22 previously healthy children aged 3-15yrs (largest of the series) who developed prolonged and recurrent refractory seizures occurring 2-14 days (median 5 days) after fever onset.
Pathophysiology
Absence of either encephalitic changes in neuroimaging,marked CSF leukocytosis or inflammatory changes on biopsy suggests that the pathological process is not one of inflammation. The clinical course is characterised by intractable recurrent/prolonged seizures suggesting neuronal hyperexcitation as the underlying cause.It is possible that the pathogenesis is immune mediated.
Clinical characteristics
-
The condition occurs in previously healthy normally developing children aged 3-15 years.
-
Characterised by an acute convulsive status epilepticus following a short febrile episode without any evidence of cns infection or inflammation.
-
The status epilepticus is highly pharmacoresistant and can persist for more than a month
-
The seizures are characteristically bilateral perisylvian with propagation to the frontal lobes and are extremely frequent and refractory
-
The acute phase is followed by a chronic pharmacoresistant epilepsy associated with severe cognitive impairment mainly involving language, memory and behaviour.
-
There is no latent period between the progression from acute to chronic phase.
Neurophysiology
-
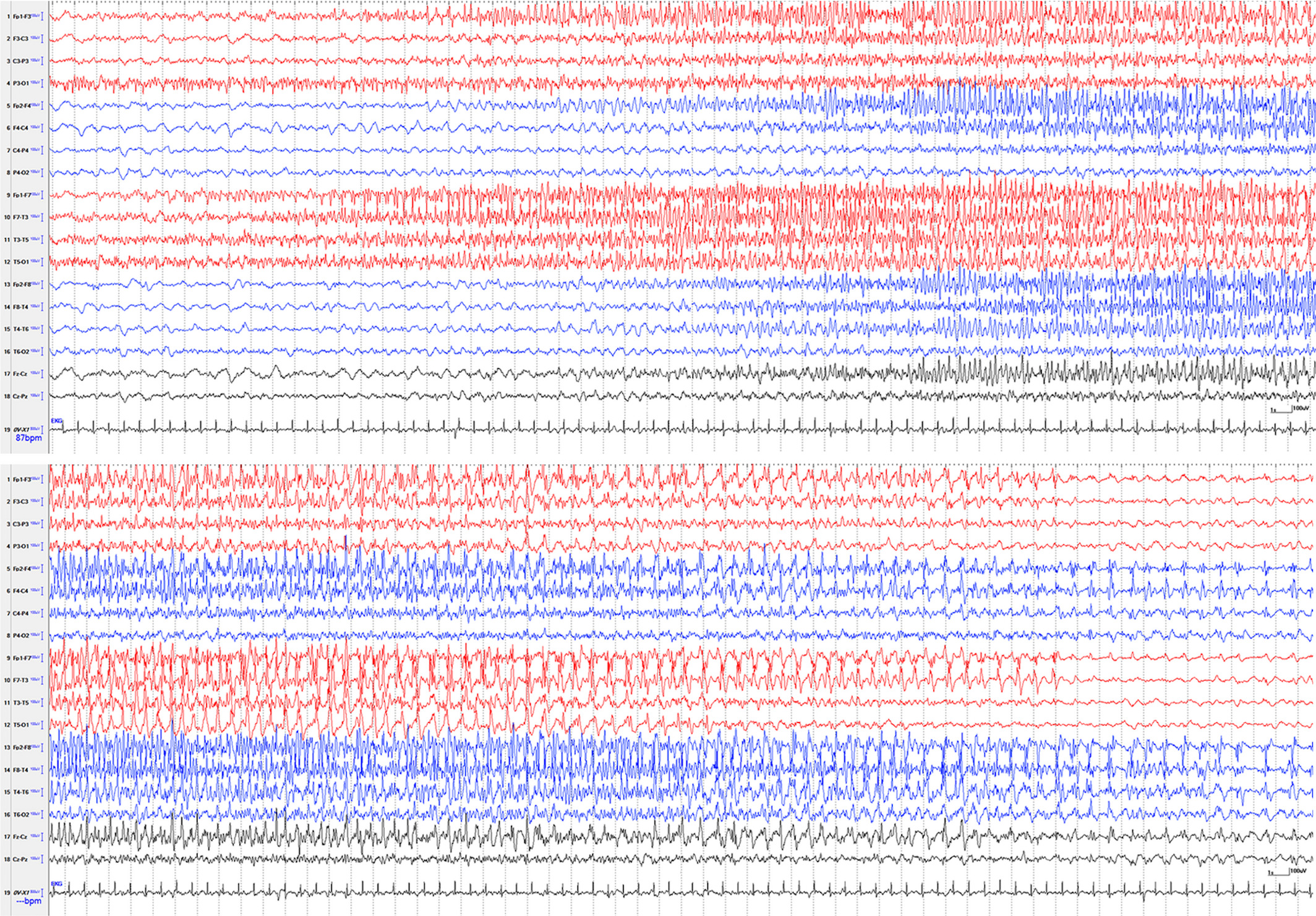
EEG shows diffuse slowing or multifocal discharges
-
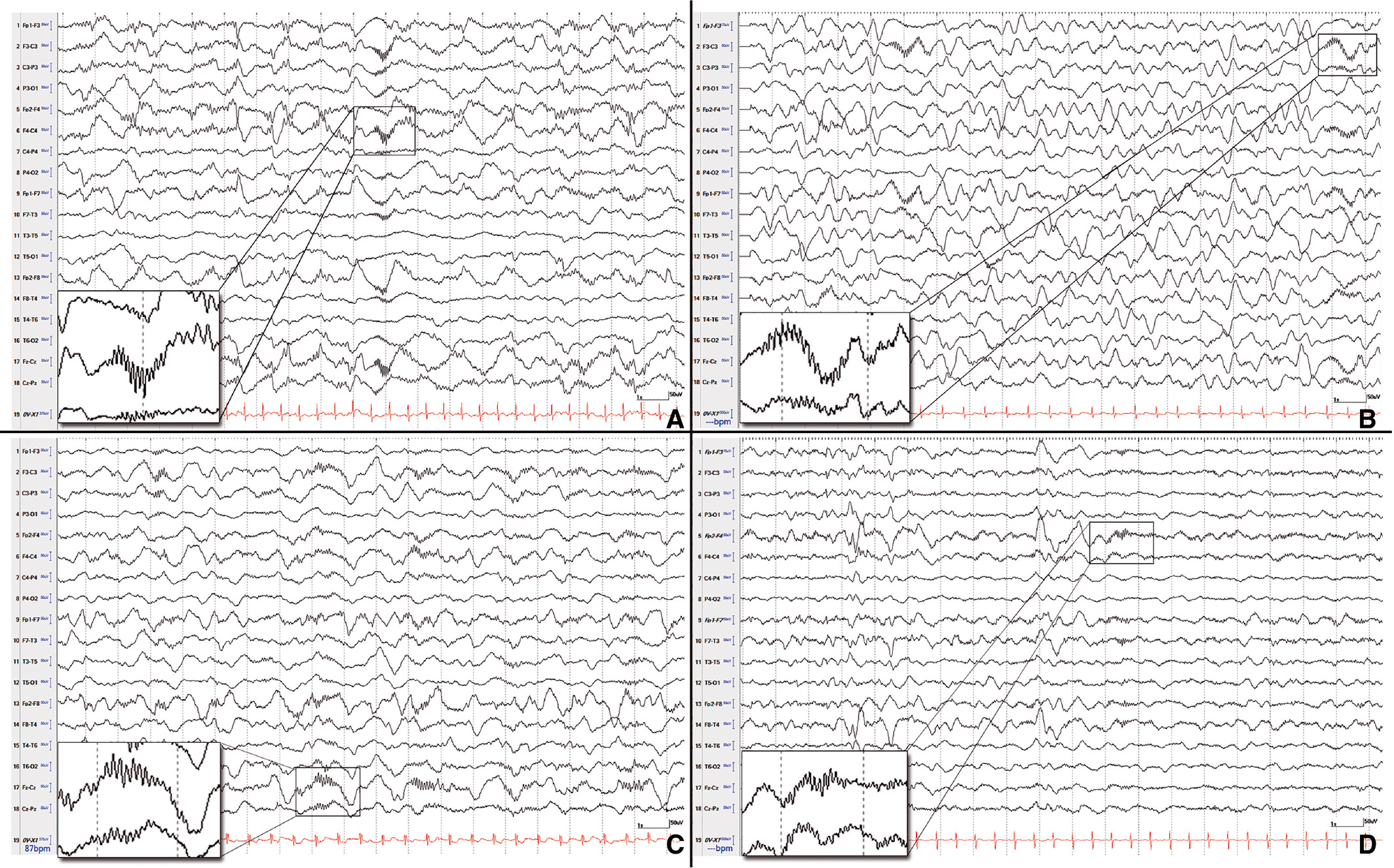
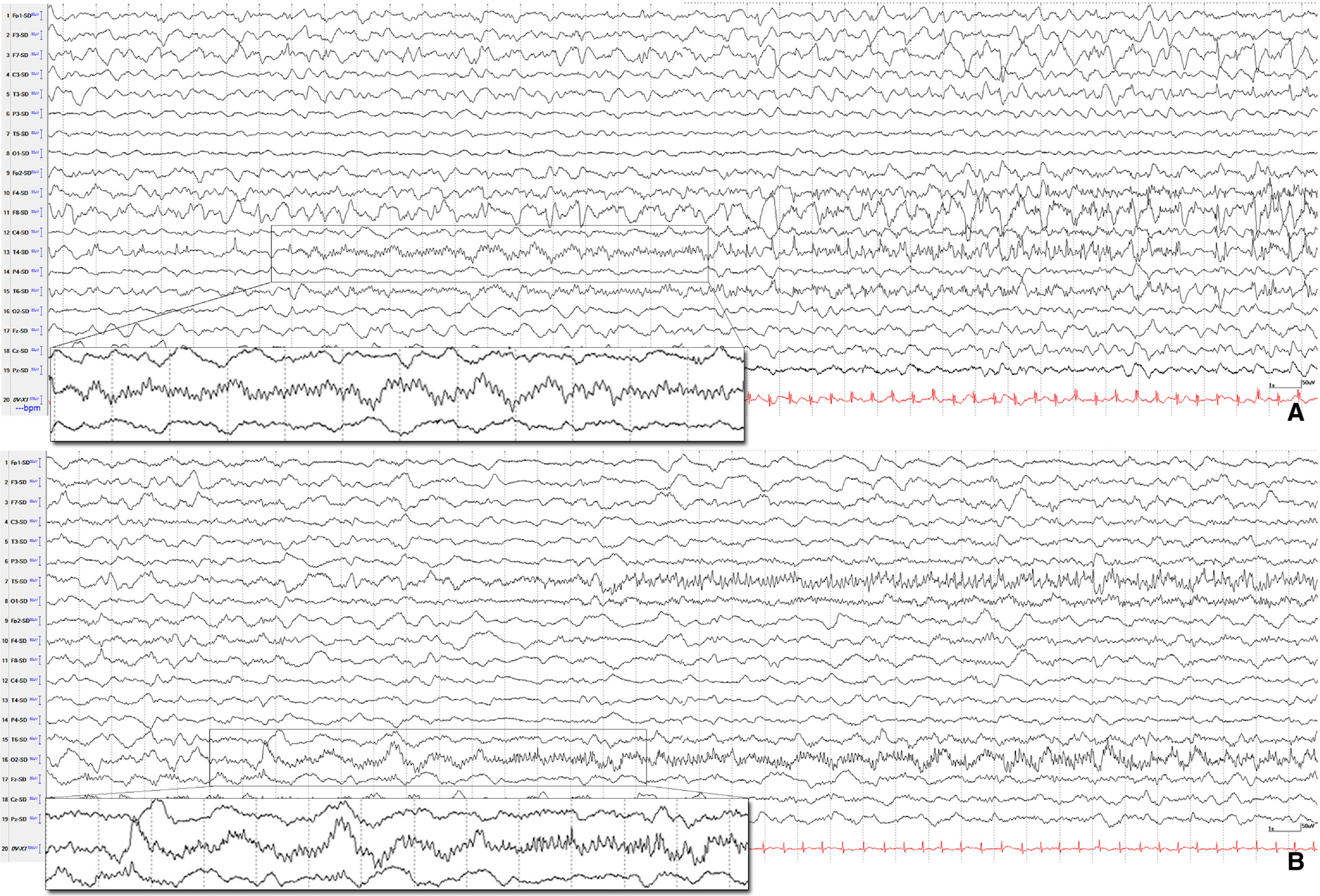
Extreme delta brush (EDB) in the background is frequently seen in the acute presentation[7]
-
prolonged focal fast activity and hemispheric shifting ictal activity is characteristic and is a potential early biomarker in patients with FIRES[7]
Neuroimaging
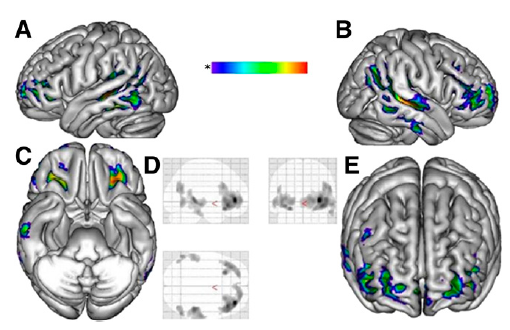
Plain MRI is often normal, although selective bilateral hippocampal abnormalities including atrophy and hypersignal have been reported.18F-FDG PET studies[8] have shown widepsread interictal hypometabolic network including the temporoparietal and orbitofrontal cortices bilaterally. The hypometabolic areas corresponded to the electroclinical seizures involving the temporofrontal cortex bilaterally as well as to the neuropsychologic findings.
Neuropsychology
Neuropsychological deficits mainly involve language, frontal functions, behaviour and memory
FIRES and NORSE
An consensus definition of FIRES proposed by a group of experts in 2018[9] excludes most cases of febrile status epilepticus in children (prolonged febrile convulsions), as febrile seizures usually occur in children who have onset of fever <24 hours prior to onset of seizures or whose fever is recognized only after the onset of seizures. New‐onset refractory status epilepticus(NORSE) is a clinical presentation, not a specific diagnosis, in a patient without active epilepsy or other preexisting relevant neurological disorder, with new onset of refractory status epilepticus without a clear acute or active structural, toxic, or metabolic cause.
Treatment
-
FIRES is characteristically highly refractory to treatment.
-
The efficacy of ketogenic diet as an alternative to pharmacotherapy in FIRES has been reported with favourable outcomes[10][11]. There are no randomized controlled trials available on the use of the ketogenic diet in status epilepticus[reference needed].
-
Deep brain stimulation of the centromedian thalamic nuclei (CMN-DBS) has been reported in some cases with where generalised seizures have been abolished but did not have a lasting effect on focal seizures burden[12]
-
There are also case reports on the use of Anakinra (a recombinant version of the human interleukin-1 receptor antagonist) in FIRES but with variable outcomes[12]
-
Gofshteyn et al.(2017) reported an open label case series where cannabadiol (Epidiolex, GW Pharma) was used alongside other anti-seizure medications on emergency or expanded investigational protocols in either the acute or chronic phase of illness and showed improvement in seizure frequency and duration[13]
References
[PMID: 22004046] [DOI: 10.1111/j.1528-1167.2011.03293.x]
[PMID: 14467623] [DOI: 10.1093/brain/84.4.680]
[PMID: 16469483] [DOI: 10.1016/j.eplepsyres.2006.01.002]
[PMID: 15832606] [DOI: 10.1177/08830738050200030301]
[PMID: 17008042] [DOI: 10.1016/j.braindev.2006.08.005]
[PMID: 20345937] [DOI: 10.1111/j.1528-1167.2010.02535.x]
[PMID: 28555777] [DOI: 10.1111/epi.13801]
[PMID: 21149491] [DOI: 10.2967/jnumed.110.077214]
[PMID: 29399791] [DOI: 10.1111/epi.14016]
[PMID: 20813015] [DOI: 10.1111/j.1528-1167.2010.02703.x]
[PMID: 19191829] [DOI: 10.1111/j.1469-8749.2008.03216.x]
[PMID: 31446001] [DOI: 10.1016/j.ejpn.2019.08.001]
[PMID: 27655472] [DOI: 10.1177/0883073816669450]
Cite this: Cite this: ICNApedia contributors.Fever induced refractory epileptic encephalopathy in school age children. ICNApedia, The Child Neurology Knowledge Environment. 30 June 2024. Available at: https://icnapedia.org/knowledgebase/articles/fever-induced-refractory-epileptic-encephalopathy-in-school-age-children Accessed 30 June 2024.