Overview
Pantothenate kinase-associated neurodegeneration (PKAN) is a rare form of neurodegeneration with brain iron accumulation (NBIA), with an estimated prevalence of 1:1,000,000 (Hayflick et al., 2006). PKAN is caused by mutations in the PANK2 gene (Zhou et al., 2001), which encodes the enzyme pantothenate kinase 2. This enzyme plays a crucial role in the first regulatory step of coenzyme A biosynthesis, essential for intermediary and fatty acid metabolism.
Clinical Presentation
-
Classic Early-Onset Form:
- Occurs in approximately 75% of PKAN cases.
- Begins in infancy with slow development and bilateral pyramidal tract signs, often initially resembling cerebral palsy.
- Between ages 5 and 10, children experience regression characterized by a decline in motor and language abilities and asymmetrical lower limb dystonia.
- Cognitive deterioration is variable, often following a step-like pattern of skill loss, stabilization, and subsequent deterioration.
- Progressive disease may lead to status dystonicus, pigmentary retinopathy, and other eye signs (Egan et al., 2005). Acanthocytes may be present in the blood film.
- Diagnosis is typically suggested by characteristic MRI findings and confirmed through genetic testing.
-
Juvenile Form:
- Less common and often initially diagnosed as a psychiatric disorder.
- Early symptoms may include hyperactivity, impulsivity, obsessive-compulsive disorder, vocal and motor tics, depression, and anxiety.
- A case described by Scarano et al. (2002) involved a patient who began stuttering at age 10 and developed an unsteady gait and frequent falls by age 17. Symptoms progressed to include motor tics, repetitive movements, compulsive behavior, vocalizations, hyperactivity, impulsiveness, and cognitive impairment. Diagnosis was made upon observing the typical 'eye of the tiger' sign on MRI (Scarano et al., 2002).
Clinical Features
- Oromandibular Dystonia: May include tongue mutilation and action-induced dystonic opisthotonus.
- Movement Disorders: Parkinsonism, choreoathetosis, and other movement disorders may occur.
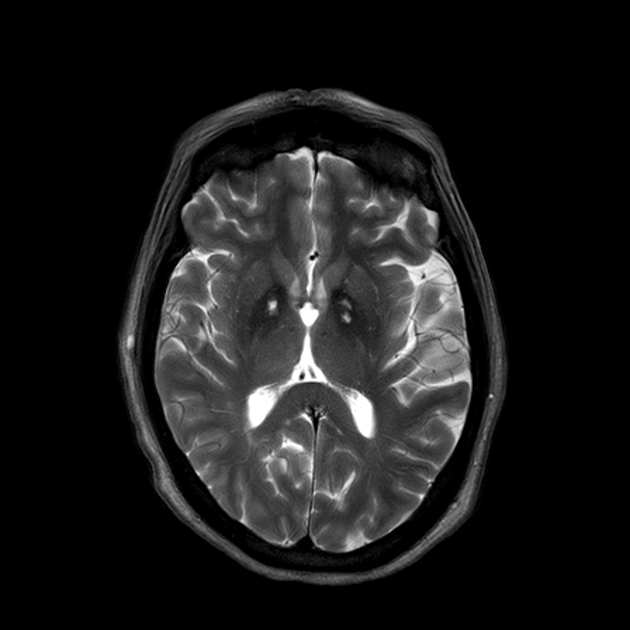
MRI Findings
- The hallmark MRI finding in PKAN is the 'eye of the tiger' sign seen on T2-weighted sequences, characterized by hypointensity of the globus pallidus with a centrally located region of hyperintensity. Pathologically, the low signal corresponds to abnormal iron deposition, and the high signal corresponds to gliosis, vacuolisation and increased water content.
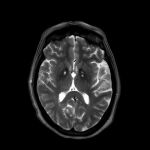
- Pathologically, this corresponds to an area of neuronal depletion and tissue rarefaction.
- Early in the disease, only hypointensity of the globus pallidus may be present, potentially leading to suspicion of a mitochondrial disorder or other metabolic problem.
- The 'eye of the tiger' sign can be found in pre-symptomatic, mutation-positive children identified after a sibling's diagnosis (Hayflick et al., 2001).
- Caution is advised in interpreting this sign due to potential mimics, such as membrane protein-associated neurodegeneration (MPAN), COASY protein-associated neurodegeneration (CoPAN), carbon monoxide poisoning survivors, multiple system atrophy, and neuroferritinopathy (Hogarth, 2015).
References
- Egan RA, Weleber RG, Hogarth P, et al. (2005) Neuro-ophthalmologic and electroretinographic findings in pantothenate kinase-associated neurodegeneration (formerly HallervordenSpatz syndrome). Am J Ophthalmol 140: 267–74.
- Hayflick SJ, Hartman M, Coryell J, et al. (2006) Brain MRI in neurodegeneration with brain iron accumulation with and without PANK2 mutations. Am J Neuroradiol 27: 1230–3.
- Hayflick SJ, Penzien JM, Michl W, et al. (2001) Cranial MRI changes may precede symptoms in Hallervorden-Spatz syndrome. Pediatr Neurol 25: 166–9.
- Scarano V, Pellecchia MT, Filla A, Barone P (2002) Hallervorden-Spatz syndrome resembling a typical Tourette syndrome. Mov Dis 17: 618–20.
- Hogarth P (2015) Neurodegeneration with brain iron accumulation: diagnosis and management. J Mov Disord 8: 1–13.
- Zhou B, Westaway SK, Levinson B, et al. (2001) A novel pantothenate kinase gene (PANK2) is defective in Hallervorden-Spatz syndrome. Nat Genet 28: 345–9.
Related Articles
Beta-propeller protein-associated neurodegeneration (BPAN)
2024-06-01 06:41:32
PLA2G6-Associated Neurodegeneration
2024-05-31 05:26:34