Neonatal seizures
- Neonatal epileptic seizures occur from birth to the end of the neonatal period.
- The neonatal period is defined as the first 28 days of life of a full-term infant.
- Most neonatal seizures are acute symptomatic seizures caused by an acute illness such as hypoxic–ischaemic encephalopathy, stroke or infection.
- seizures are the most common and important sign of acute neonatal encephalopathy
- neonatal seizures are a major risk for death or subsequent neurological disability and, by themselves, may contribute to an adverse neuro-developmental outcome.
Classification
- The ILAE Commission (1989)[1] broadly classifies the neonatal seizures among ‘epilepsies and syndromes undetermined as to whether they are focal or generalised’ under the subheading ‘with both generalised and focal seizures’
- In the ILAE (2010)[2] revised classification neonatal seizures are no longer regarded as a separate entity.
Clinical features
Five main types of seizures are recognised[3]
- subtle seizures (50%)
- tonic seizures (5%)
- clonic seizures (25%)
- myoclonic seizures (20%)
- non-paroxysmal repetitive behaviours
Subtle seizures
- most common type; subtle clinical manifestations
- ocular movements (random and roving eye movements to sustained conjugate tonic deviation with or without jerking)
- Eyelid blinking or fluttering, eyes rolling up, eye opening, fixation of a gaze or nystagmus may occur alone or with other ictal manifestations
- oral–buccal–lingual movements (sucking, chewing, smacking and tongue protrusions)
- progression movements (rowing, swimming, pedalling, bicycling, thrashing or struggling movements)
- complex purposeless movements (sudden arousal with episodic limb hyperactivity and crying)[4]
Clonic seizures
- rhythmic jerks that may localise in a small part of the face or limbs, axial muscles and the diaphragm, or be multifocal or hemiconvulsive.
- Multifocal clonic seizures may migrate to other body parts or other limbs. Todd’s paresis follows prolonged hemiconvulsions.
Tonic seizures
- manifest with sustained contraction of facial, limb, axial and other muscles
- may be focal, multifocal or generalised, symmetrical or asym-metrical
- Truncal or limb tonic extensions imitate decerebrate or decorticate posturing (occur particularly in pre-term infants and have a poor prognosis because they frequently accompany intra-ventricular haemorrhage)[5]
Myoclonic seizures
- rapid, single or arrhythmic repetitive jerks. They may affect a finger, a limb or the whole body. They may mimic Moro reflex and startling responses
- more frequently in pre-term than in full-term infants indicating, if massive, major brain injury and poor prognosis[6].
- healthy pre-term and, although rarely, full-term neonates may have abundant myoclonic movements during sleep
- Neonates have cortical, reticular and segmental types of myoclonus, similar to adult forms (Scher, 1985).
Spasms
- flexion or extension spasms similar to those of West syndrome are rare
- slower than myoclonic and clonic seizures and faster than tonic seizures
Autonomic ictal manifestations
- autonomic ictal manifestations commonly occur with motor manifestations in 37% of subtle seizures
- paroxysmal changes of heart rate, respiration and systemic blood pressure, salivation, pupillary changes
- Apnoea, as an isolated seizure phenomenon unaccompanied by other clinical epileptic features, is rare[6]
The duration of neonatal seizures is usually brief (10 s to 1–2 min) and repetitive with a median of 8 min in between each seizure. Longer seizures and status epilepticus develop more readily at this age, but convulsive neonatal status epilepticus is not as severe as that of older infants and children.
Non-epileptic neonatal seizures
- show clinical similarities to reflex behaviours of the neonates, but are not associated with ictal EEG discharges and commonly correlate with diffuse abnormal brain processes such as hypoxic ischaemic encephalopathy and a poor short-term outcome.
- considered as ‘brain-stem release phenomena’- exaggerated reflex behaviours due to abnormal release of brain-stem tonic mechanisms from cortical control
Etiology
- hypoxia-ischemia (most common cause)
- haemorrhage (spontaneous/traumatic), cerebral infarction, cortical vein thrombosis
- trauma
- infections
- metabolic
- hypoglycaemia
- neonates of diabetic mothers
- pancreatic disease
- Glucogen storage disease (idiopathic)
- Hypocalcaemia
- early, in first 2 or 3 days, mainly in preterm neonates with prenatal or perinatal insults
- late, at 5–14 days, is mainly nutritional; maternal hyperparathyroidism; DiGeorge's syndrome
- Hypomagnesaemia (may accompany or occur independently of hypocalcaemia)
- Hyponatraemia (maily nutritional or iatrogenic)
- Inborn errors of metabolism
- Congenital and early infantile Neuronal ceroid lipofuscinosis (NCL)
- drug withdrawal
- inadvertent injection of local anaesthetics during delivery
- benign neonatal seizures (familial and non-familial)
Electroencephalography
interictal EEG
- epileptogenic spikes or sharp slow wave foci on interictal EEG are not reliable markers
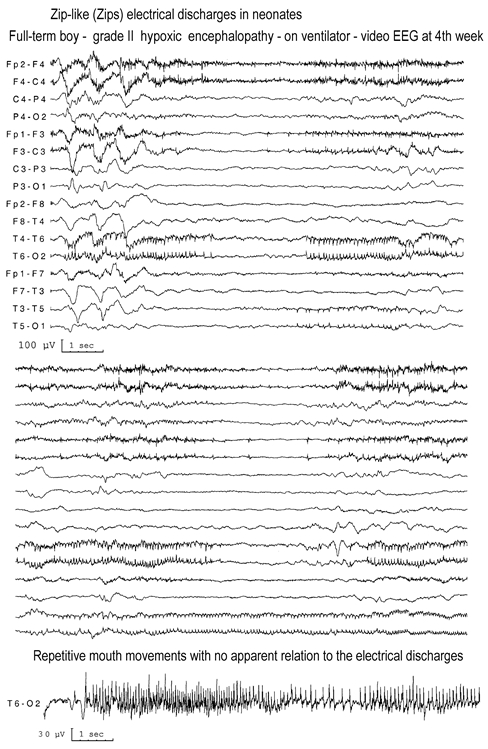
- Zip-like electrical discharges (high frequency rapid spikes of accelerating and decelerating speed, starting from various locations, terminating in one while continuing in another) in severe hypoxia
 Zip-like electrical discharges
Zip-like electrical discharges
- Theta pointu alternant in benign neonatal convulsions
 Theta pointu alternant
Theta pointu alternant - Quasi-periodic focal or multifocal pattern in neonatal herpes simplex encephalitis
- persistently focal sharp or slow waves in localised lesions.
- Periodic complexes in glycine encephalopathy
- suppression–burst pattern in neonatal epileptic encephalopathies
 suppression-burst pattern
suppression-burst pattern- relatively common in neonatal period
- can be induced by drugs[9]
- usually transient in ischemic encephalopathy
- stable lasting for more than 2 weeks in Ohtahara syndrome and early myoclonic encephalopathy
Ictal EEG
- may be focal or multifocal appearing in a normal or abnormal background and vary in frequency, amplitude and morphology in the same or subsequent seizures
- paroxysms consist of
- repetitive waves with a predominant beta, alpha, theta and delta range or a mixture of all of varying frequency
- spikes, sharp or saw tooth or sinusoidal waves (monomorphic or polymorphic) ranging in amplitude from very low to very high
- patterns associated with severe encephalopathies and usually poor prognosis
- Alpha seizure discharges - sustained and rhythmic activity of 12 Hz and 20–70 μV in the centrotemporal regions
- discharges of low voltage and long duration which are highly localised on one side and shows little tendency to spread
Stimulus-evoked electrographic patterns
- electrographic seizures are elicited by tactile or painful stimulation (with or without concomitant clinical ictal manifestations)
- represent an abnormal form of cortical reactivity to sensory stimuli in the developing brain[10]
- most neonates with these patterns have significant diffuse or multifocal damage to the neocortex
Electroclinical dissociation
- clinical component of a seizure occurs at times with or without an electrical correlate
- ‘decoupling response’ - commonly seen after starting AEDs where AEDs may suppress the clinical manifestations of seizures but not the EEG ictal discharge
- may arise from foci not consistently echoed by surface electrodes[11]
Differential diagnosis
Prognosis
- depends on the underlying cause[5]
- Indicators of bad prognosis
- Severe hypoxia–ischaemia
- Severe congenital malformations of cortical development and meningoencephalitis
- Subtle and generalised tonic seizures
- Nearly flat EEG or of very low voltage and discontinuous EEG with bursts of high-voltage spikes and slow activity
- Indicators of good prognosis
- Hypocalcaemia (alimentary type) and other transient metabolic changes
- Extracranial infections with seizures (otitis, pneumonia, gastroenteritis, etc.)
- Benign familial and non-familial convulsions
- Clonic seizures that are short and infrequent
- Normal inter-ictal EEG
- Indicators of intermediate or guarded prognosis
- Moderately severe central nervous system (CNS) infections or malformations
- Most of the intracranial haemorrhages or infarctions
- More serious metabolic CNS disturbances
- EEG persistence of immature patterns
- Frequent or prolonged clonic seizures and clonic status epilepticus
Management
Investigations
- Neuroimaging
- CT, MRI, Cranial USS
- EEG
- Blood tests
- CSF studies
Treatment
 This section needs significant updating in light of recent advances in this field(LIST).
This section needs significant updating in light of recent advances in this field(LIST).
~~AUTHORS:off~~
There is limited evidence regarding the best pharmacologic treatment for neonatal seizures. World Health Organisation recommends electrographic seizures should be treated in the same way as clinical seizures[17].
- phenobarbital
- often recommended as first-line treatment[18]
- recommended as first line treatment in the UK[19]
- included in RCTs of first-line treatment of neonatal seizure
- most studied anti-epileptic medication in animals
- historical precedence as the first-line antiepileptic drug for neonates
- extremely limited evidence on the effect of phenobarbital on long-term neonatal neurodevelopment
- U.S. Food and Drug Administration (FDA) has never approved phenobarbital for use in any patient population[20]
- animal studies have raised concerns that neonatal phenobarbital exposure induces neuronal apoptosis, disruption of synaptic development in the striatum, and other behavioral deficits[21]
- Levetiracetam
- effective as second-line treatments for neonatal seizures that are unresponsive to phenobarbital
- FDA-approved for children as young as one-month of age[22]
- efficacy and safety profile has not been adequately studied in term or preterm neonates within the first month of life
- current literature suggests loading doses of 10 to 20 mg/kg are appropriate and effective in neonates, with a maintenance dose range of 10 to 80 mg/kg/day divided twice daily[23]
- dosing of 40–50mg/kg bolus has also been suggested [24]
- a recent open labelled RCT (Level III neonatal unit; 100 neonates) used Levetiracetam (20 mg/kg) or Phenobarbitone (20 mg/kg) intravenously and concluded that Levetiracetam achieves better control than Phenobarbitone for neonatal clinical seizures when used as first-line antiepileptic drug, and is not associated with adverse drug reactions[25]
- phenytoin/fosphenytoin
- effective as second-line treatments for neonatal seizures that are unresponsive to phenobarbital
- requires frequent blood-level monitoring
- erratic oral absorption & needs 6-8hrly oral dosing
- lidocaine
- effective as second-line treatments for neonatal seizures that are unresponsive to phenobarbital.
- narrow therapeutic window and the potential to cause cardiac arrhythmias or hypotension
- can induce seizures at high doses
- may be considered in status epilepticus if phenytoin was no previously given
- Benzodiazepines (midazolam)
- sedation is a serious side effect
- may be considered as a second- or third-line therapy choice, especially in already intubated neonates
Other considerations
- consider pyridoxine challenge when other antiepileptics provide no response
- minimal data for many antiepileptics including topiramate, which is being increasingly used in neonates
- steroids and / or Vigabatrin are considered in epileptic spasms
- Low-dose carbamazepine (CBZ) should be considered as first-line treatment for benign familial neonatal epilepsy (BNFE), even in cases of status epilepticus[26]
- there is equipoise on levetiracetam vs phenobarbitone as first line treatment[27]
- The 2011 World Health Organization (WHO) guidelines for neonatal seizures[17] and the 2010 Queensland Maternity and Neonatal Clinical Guidelines for neonatal seizures[28] recommend phenobarbital as the first-line agent for treatment of neonatal seizures, followed by phenytoin, and then benzodiazepines
References
[PMID: 9546495] [DOI: 10.1016/s0013-4694(97)00061-8]
Discussion