Paroxysmal sympathetic hyperactivity in a child with High Grade Glioma post resection surgery.
Sarvesh Kohli, Apoorv Saxena, Subir Dey, Sudip Sengupta, TVSVGK Tilak, Biju M John, VISHAL SONDHI, Sachendra Badal
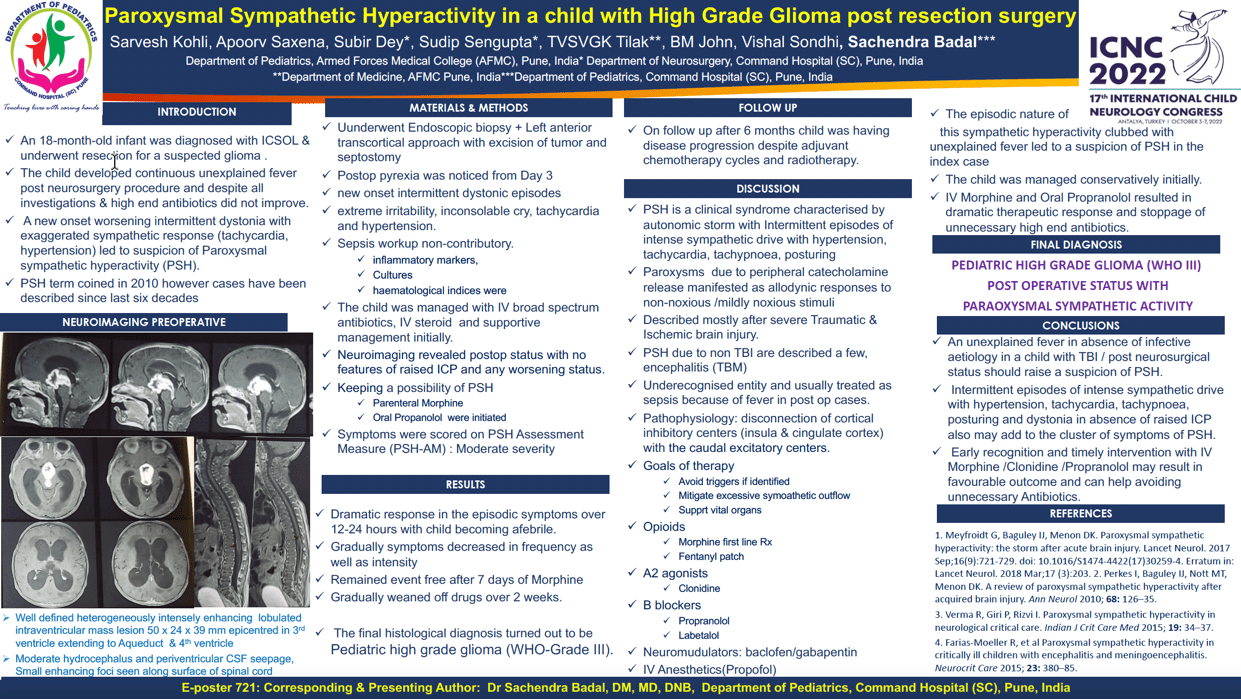
Objective We present child diagnosed with ICSOL who underwent resection of a brain tumour. The child developed continuous unexplained fever post neurosurgical procedure. A new onset worsening intermittent dystonia with exaggerated sympathetic response led to suspicion of Paroxysmal Sympathetic Hyperactivity (PSH). Methods An 18-month-old toddler diagnosed with ICSOL underwent resection for a suspected glioma .Postop pyrexia was noticed from Day 3 which was followed by appearance of new onset intermittent dystonic episodes associated with extreme irritability, inconsolable cry, tachycardia and hypertension. Sepsis workup including inflammatory markers, cultures and hematological indices were non-contributory. Neuroimaging revealed postop status with no features of raised ICP and any worsening status. The child was managed with IV broad spectrum antibiotics, IV steroid and supportive management initially. The episodic nature of this sympathetic hyperactivity clubbed with unexplained fever led to a suspicion of PSH. Results There was a dramatic therapeutic response (fever abated over 12-24 hours) with IV Morphine and oral Propranolol leading to stoppage of unnecessary prolonged high end antibiotics. Gradually episodic symptoms decreased in frequency as well as intensity and then remained event free after 7 days of Morphine and subsequently gradually weaned off all drugs over 15 days. Conclusion An unexplained fever in absence of infective aetiology with traumatic brain injury/post neurosurgical status should raise suspicion of PSH. The intermittent episodes of intense sympathetic drive and dystonia in absence of raised ICP also add to cluster of symptoms. Early recognition and timely intervention with IV Morphine /Clonidine /Propranolol may result in favorable outcome.
Keywords: Paroxysmal sympathetic hyperactivity in a child with High Grade Glioma
Sarvesh Kohli
ARMED fORCES mEDICAL cOLLEGE
India
Apoorv Saxena
AFMC
India
Subir Dey
COMMAND HOSPITAL SC
India
Sudip Sengupta
COMMAND HOSPITAL SC
India
TVSVGK Tilak
AFMC
India
Biju M John
AFMC
India
Objective We present child diagnosed with ICSOL who underwent resection of a brain tumour. The child developed continuous unexplained fever post neurosurgical procedure. A new onset worsening intermittent dystonia with exaggerated sympathetic response led to suspicion of Paroxysmal Sympathetic Hyperactivity (PSH). Methods An 18-month-old toddler diagnosed with ICSOL underwent resection for a suspected glioma .Postop pyrexia was noticed from Day 3 which was followed by appearance of new onset intermittent dystonic episodes associated with extreme irritability, inconsolable cry, tachycardia and hypertension. Sepsis workup including inflammatory markers, cultures and hematological indices were non-contributory. Neuroimaging revealed postop status with no features of raised ICP and any worsening status. The child was managed with IV broad spectrum antibiotics, IV steroid and supportive management initially. The episodic nature of this sympathetic hyperactivity clubbed with unexplained fever led to a suspicion of PSH. Results There was a dramatic therapeutic response (fever abated over 12-24 hours) with IV Morphine and oral Propranolol leading to stoppage of unnecessary prolonged high end antibiotics. Gradually episodic symptoms decreased in frequency as well as intensity and then remained event free after 7 days of Morphine and subsequently gradually weaned off all drugs over 15 days. Conclusion An unexplained fever in absence of infective aetiology with traumatic brain injury/post neurosurgical status should raise suspicion of PSH. The intermittent episodes of intense sympathetic drive and dystonia in absence of raised ICP also add to cluster of symptoms. Early recognition and timely intervention with IV Morphine /Clonidine /Propranolol may result in favorable outcome.
Keywords: Paroxysmal sympathetic hyperactivity in a child with High Grade Glioma
Sarvesh Kohli
ARMED fORCES mEDICAL cOLLEGE
India
Apoorv Saxena
AFMC
India
Subir Dey
COMMAND HOSPITAL SC
India
Sudip Sengupta
COMMAND HOSPITAL SC
India
TVSVGK Tilak
AFMC
India
Biju M John
AFMC
India
Sachendra Badal
COMMAND HOSPITAL/AFMC India
COMMAND HOSPITAL/AFMC India