Chylous blood in an infant with febrile encephalopathy: Clues to metabolic etiology (Very Long Chain Acyl CoA Dehydrogenase Deficiency)
Bishwo Kunwar, Sushant Ghimire, Prerna Guleria, Amit Devgan, Vishal Sondhi, Sachendra Badal
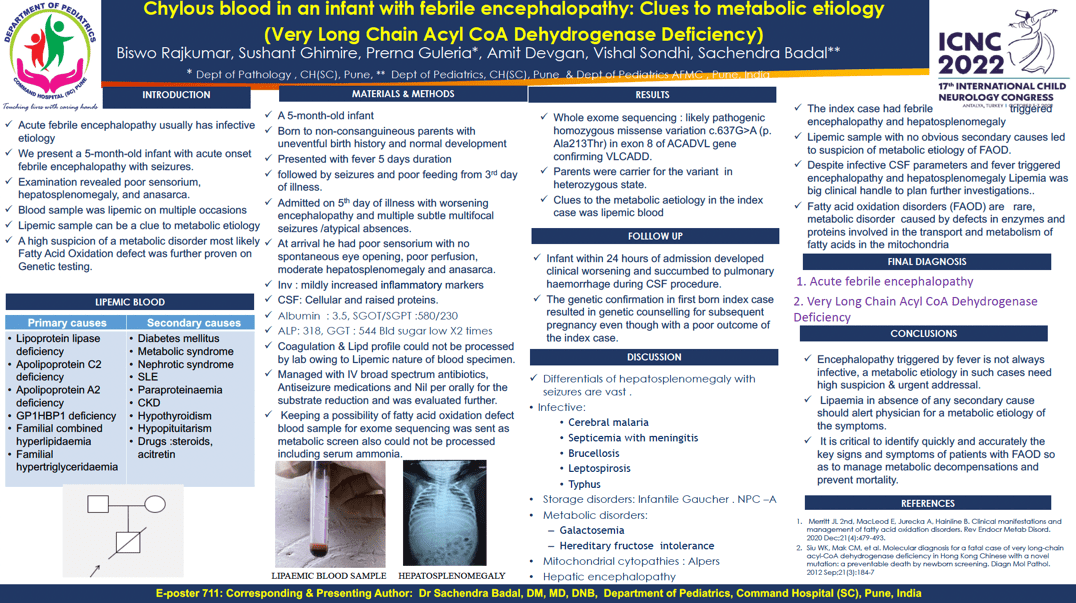
Objective An infant with acute onset febrile encephalopathy and seizures admitted with poor sensorium, hepatosplenomegaly and anasarca. Blood sample twice could not be processed due to lipemia. Genetic evaluation confirmed Very Long Chain Acyl CoA Dehydrogenase Deficiency (VLCADD), a fatty acid oxidation defect. Methods A 5-month-old infant born to non-consanguineous parents with uneventful birth history and normal development presented with Short febrile illness fever, seizures and poor feeding. Admitted with worsening encephalopathy and multiple subtle multifocal seizures .On exam had poor sensorium with no spontaneous eye opening, poor perfusion, moderate hepatosplenomegaly and anasarca. Investigations revealed mildly increased inflammatory markers with a cellular CSF and raised proteins. Serum albumin was very low with mildly raised transaminases. Coagulation profile could not be processed by lab owing to Lipemic nature of blood specimen. The child was managed conservatively and was evaluated further. Keeping a possibility of fatty acid oxidation defect blood sample for Exome sequencing was sent as metabolic screen also could not be processed including serum ammonia. Results Genetic evaluation revealed pathogenic homozygous missense variation of ACADVL gene confirming VLCADD. Infant developed rapid clinical worsening and succumbed to pulmonary haemorrhage. Clues to the metabolic etiology in the index case was lipemic blood (in absence of any secondary causes like diabetes, hypothyroidism) despite infective CSF parameters and fever triggered encephalopathy. Conclusion Encephalopathy triggered by fever is not always infective, metabolic etiology in such cases need high suspicion & urgent addressal. Lipaemia in absence of secondary cause should alert physician for a metabolic etiology.
Keywords: Very Long Chain Acyl CoA Dehydrogenase Deficiency, Lipemia, Febrile encephalopathy
Bishwo Kunwar
ARMED fORCES mEDICAL cOLLEGE
India
Sushant Ghimire
AFMC
India
Prerna Guleria
COMMAND HOSPITAL SC
Objective An infant with acute onset febrile encephalopathy and seizures admitted with poor sensorium, hepatosplenomegaly and anasarca. Blood sample twice could not be processed due to lipemia. Genetic evaluation confirmed Very Long Chain Acyl CoA Dehydrogenase Deficiency (VLCADD), a fatty acid oxidation defect. Methods A 5-month-old infant born to non-consanguineous parents with uneventful birth history and normal development presented with Short febrile illness fever, seizures and poor feeding. Admitted with worsening encephalopathy and multiple subtle multifocal seizures .On exam had poor sensorium with no spontaneous eye opening, poor perfusion, moderate hepatosplenomegaly and anasarca. Investigations revealed mildly increased inflammatory markers with a cellular CSF and raised proteins. Serum albumin was very low with mildly raised transaminases. Coagulation profile could not be processed by lab owing to Lipemic nature of blood specimen. The child was managed conservatively and was evaluated further. Keeping a possibility of fatty acid oxidation defect blood sample for Exome sequencing was sent as metabolic screen also could not be processed including serum ammonia. Results Genetic evaluation revealed pathogenic homozygous missense variation of ACADVL gene confirming VLCADD. Infant developed rapid clinical worsening and succumbed to pulmonary haemorrhage. Clues to the metabolic etiology in the index case was lipemic blood (in absence of any secondary causes like diabetes, hypothyroidism) despite infective CSF parameters and fever triggered encephalopathy. Conclusion Encephalopathy triggered by fever is not always infective, metabolic etiology in such cases need high suspicion & urgent addressal. Lipaemia in absence of secondary cause should alert physician for a metabolic etiology.
Keywords: Very Long Chain Acyl CoA Dehydrogenase Deficiency, Lipemia, Febrile encephalopathy
Bishwo Kunwar
ARMED fORCES mEDICAL cOLLEGE
India
Sushant Ghimire
AFMC
India
Prerna Guleria
COMMAND HOSPITAL SC
Sachendra Badal
AFMC India
AFMC India