Subcutaneous immunoglobulin in anti-HMGCR myopathy with children for long-term maintenance
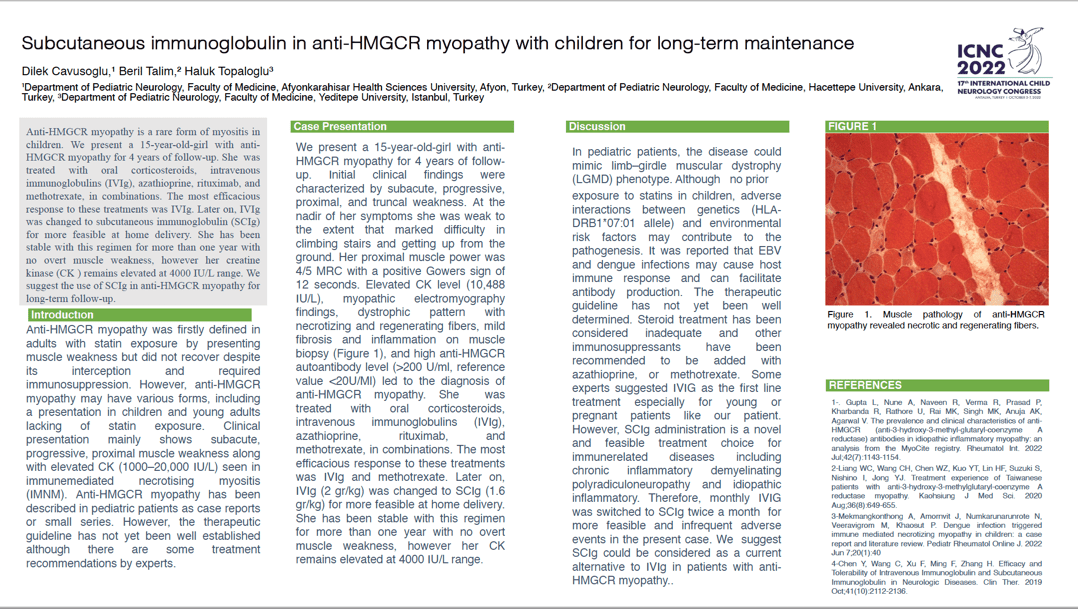
Anti-3-hydroxy-3-methylglutaryl-coenzyme A reductase (HMGCR) immune-mediated necrotizing myopathy is a subtype of idiopathic inflammatory myopathy which may be associated with statin exposure. It presents with severe proximal muscle weakness, high creatine kinase levels and muscle fiber necrosis. Diagnosis is based on muscle biopsy features (predominantly necrotizing myopathy) and the presence of anti-HMGCR autoantibodies. To date, knowledge of anti-HMGCR myopathy in children has been reported as small case series or single cases. We present a 15-year-old-girl with anti-HMGCR myopathy for 4 years of follow-up. Initial clinical findings were characterized by subacute, progressive, proximal, and truncal weakness. At the nadir of her symptoms she was weak to the extent that marked difficulty in climbing stairs and getting up from the ground. Her proximal muscle power was 4/5 MRC with a positive Gowers sign of 12 seconds. Elevated creatine kinase level (10,488 IU/L), dystrophic pattern with necrotizing and regenerating fibers, mild fibrosis and inflammation on muscle biopsy, and high anti-HMGCR autoantibody level led to the diagnosis of anti-HMGCR myopathy. She was treated with oral corticosteroids, intravenous immunoglobulins (IVIg), azathioprine, rituximab, and methotrexate, in combinations. The most efficacious response to these treatments was IVIg. Later on, IVIg was changed to subcutaneous immunoglobulin (SCIg) for more feasible at home delivery. She has been stable with this regimen for more than one year with no overt muscle weakness, however her CK remains elevated at 4000 IU/L range. We suggest the use of SCIg in anti-HMGCR myopathy for long-term follow-up.
Faculty of Medicine, Afyonkarahisar Health Sciences University Turkey